I get a strange feeling of unease every time I type "ATI" and "medical" in the same sentence. I think this is because the medical section is quite strange. This section, for example, manages to be very detailed without necessarily teaching information well.

As is usual, there is a mishmash of poor word choice and incorrect facts.
- The sentence that starts with "Sound is produced ...." should be "Speech is produced..." since sound can be made without using the respiratory system by clapping, snapping, stomping etc.
- Since this is a medical course, the medical terms for parts of the body should be introduced and used consistently. The windpipe is known as the trachea, the voice box is the larynx, and the "throat" is probably the pharynx.
- Breathing is used to rid the body of excess carbon dioxide when a person or a baby exhales. Calling that "continuous purification" is needlessly complicated at best and misleading at worst.
- Many spiritual disciplines use conscious control of breathing which is a very different beast than reflexive breathing.


The copy I have of this wisdom booklet is a bit cut off at the top of one page so this section is missing a line or two. Yet again, problems occur:
- There is no vacuum within the lungs themselves during breathing. The critical vacuum occurs between the lungs and the wall of the chest.
- That vacuum keeps the lungs attached to the wall of the chest so that the volume of the lungs expands and contracts as the chest moves.
- If that vacuum fails because of a hole in a lung or a hole in the wall of the chest, one or both lungs can detach from the chest wall or collapse. When a lung collapses, it does not work at all. This is a medical emergency. A collapsed lung can be fixed by placing a tube in the chest known as a pneumothorax tube until the injury heals.
- Collapsed lungs are common in premature infants who have immature lungs. I had two pneumothorax tubes placed in my first week of life. I had no long-term consequences from the procedure except for two small scars on my chest.
- I've never heard the term "voice corridor" used before. I'd substitute "trachea and larynx" since this portion is about vocal sound production.
- The rest is reasonably correct. There's a neat demonstration people can do at home to show how the lungs work using half a plastic pop bottle, two balloons, a straw, some clay or a cork, and rubber bands. Here's a website with written instructions and a YouTube video for the visual learners. I came up with a series of adaptations to demonstrate when I taught anatomy (and because I like messing around with models....)
- You can demonstrate a collapsed lung by poking a hole in the bottle with a sharp needle or a nail.
- Let your kids try to figure out how to fix a collapsed lung.
- The trick is to fix the hole while having the chest wall under a lot of pressure so the air between the chest wall and the lungs is forced out. Doing that will create a near-vacuum.
- In real life, you would have the person exhale as hard as they can and quickly patch the hole/wound with something that is air-tight like a sheet of plastic.
- For the model, you squish the bottle hard while pushing up on the "diaphragm" and plug the hole with a wad of clay, saran-wrap or play-dough.
- You can also demonstrate choking and the Heimlich maneuver using the lung model. You can obstruct the trachea using a piece of clay. The Heimlich maneuver is essentially pushing the diaphragm upward quickly and forcefully.
- If the obstruction is small enough, the Heimlich maneuver will knock it free.
- If it is too large, you can demonstrate emergency intubation by shoving a small coffee stirrer down the trachea to bypass the obstruction.
- You can also demonstrate why the Heimlich maneuver won't work if the person can still talk, cough or make sounds. If you put a small bit of clay on one side of the trachea to model a partial obstruction, you'll see that the Heimlich maneuver does nothing but potentially injure the other person.

- This is the first section I don't have a major problem with!


- If I was using this reading while teaching, I'd be worried that I would have a bunch of hoarse students. Just ramping up the pressure of air moving through the larynx will make a person's voice louder, but will also do micro (or macro) damage to the vocal cords that will lead to a hoarse voice. Doing this repeatedly can lead to serious damage to the vocal cords.
- To make your voice louder, it's important to learn how to breathe deeply so that the lungs are filled with air. My choir teacher showed us how to breathe deeply by laying down on the floor and placing your hand just under your rib cage. As you breathe, you focus breathing so that the hand moves upward on the inhale.
- It's also important to learn how to stand upright with a neutral spine and squared shoulders to have the largest available volume of air.
- The next trick is learning how to create a smooth exhale of air using your diaphragm and abdominal muscles.
- The bit that will keep your vocal cords from being shredded is learning how to have large volumes of air moving through the vocal cords while keeping the cords as relaxed as possible. For me, I need to focus on keeping my larynx as low as possible.
- The last trick is learning how to keep your face/sinuses as open as possible to increase resonance. To me, it feels like keeping my eyes opened wide with my cheekbones raised and jaw dropped.

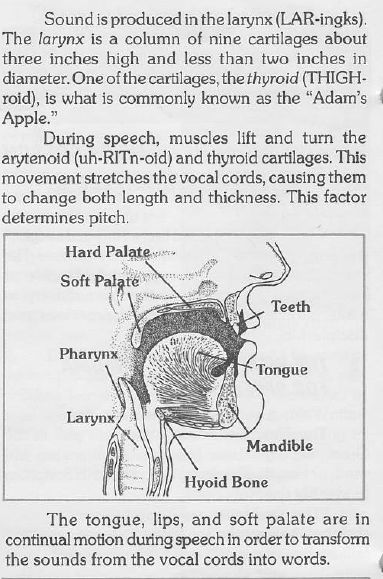
- The top illustration is odd.
- The mouth above the tongue and nose portion is right.
- The diagram is either missing the hyoid bone...or has two.
- The vocal cord fold is really difficult to see in black and white on the diagram.
- This is more a personal preference, but since they labeled the epiglottis, I would have labeled the esophagus which is the thin tube behind the cricoid cartilage and in front of the spine. The epiglottis flips down to block the trachea when we swallow so food doesn't end up in the lungs.
- Actually, sounds can be made in some sections of the vocal tract independently. Clicking sounds can be made using just the tongue. (Random factoid: English speakers do use click sounds; we use them as a method of signalling a transition in topics. English speakers find languages that do use click sounds highly confusing because we interpret the click as a topic change rather than a constant sound so our brains interpret the person speaking as changing subjects multiple times per sentence. Try reading that last few sentences aloud with a click every time you see an "S" to see the problem.)
- The second illustration has one problem: the item labeled "thyroid" should be labeled "thyroid cartilage" since the thyroid is a different organ located in front of the thyroid cartilage.
- The order that material is presented makes no sense in these booklets. This section would make the most sense if it came after the section on the lungs. Placed there, the reader would have a basic idea of how the larynx itself works before jumping into the details of speech production. Instead, it's tacked on to the end.
- I wanna know who made these illustrations.
- This illustration has a huge amount of soft tissue in front of the mandible.
- The person has really small bottom teeth which are nearly obscured by the line that labels the tongue.
- The person also has a gaping fissure that will let food pass from the back of the tongue in front of the epiglottis and settle down on top of the thyroid cartilage.
- The larynx is an area and that was covered pretty well in the previous portions. Unfortunately, the pharynx is an area, not one spot. The diagram does a horrible job of showing that.

- I like the inclusion of speech therapy in this part. I wish they had used more detail here, including a diagram that doesn't show a person making P, B, W and F sounds with their lips shut.
- The "Project" isn't a project. At best, it's an open-ended question that should take about 15-30 minutes to do. At worst, it's really a daft question.
Next up: ATI's take on Chemistry. Hopefully, I will have ID the mystery structure by then.....
As a linguist, I'm cringing at their take on "plosive" consonants. To start: 'Q' is not a simple consonant in English. The sound represented as [q] in phonetics is actually an uvular consonant and so is articulated farther back in the throat than the spot where they've put it and does not occur in English. The English 'Q' is closer to [kw] or a labialized [k] (which should have a little w superscript after it but I think that's a bit beyond my basic html abilities). And [w] is a labial-velar consonant, which means the tongue is making contact at the velum, near the back of the mouth, where the g and k are articulated, while the lips are also shaping the sound. Putting it with the labial consonants is a bit of a misnomer because it's articulated in two places at the same time. And sticking 'f' with 'p' and 'b' irritates me because while it is a labial consonant, it's technically a different place and mode of articulation than 'p' and 'b' so it doesn't always group together with those sounds.
ReplyDeleteAnd the biggest error is this: "plosive" is another term for "stop" which refers to consonants where the airflow through the mouth is completely impeded. [f] is a fricative consonant, where the airflow is mostly but not fully impeded. It is not a plosive. [w] is an approximant, which means the articulators (e.g., the tongue and the velum) come close to each other, but do not touch, and therefore the airflow is not impeded. Basically, it looks like they're defining all consonants as plosives, which is just incorrect. It would be accurate to label the consonants they've included as pulmonic (where the air for the consonants comes from the lungs), but apparently they didn't do enough research for that.
Your comment has made me happy in a way I can barely describe. I love when people with actual knowledge in an area give me more feedback!
DeleteYour explanation makes so much sense. I've been trying to make a W or F sound with my lips completely closed and with a total stop of air flow all weekend. It hasn't worked. At all. Not even a bit. :-)
Your comment has made me happy in a way I can barely describe. I love when people with actual knowledge in an area give me more feedback!
DeleteYour explanation makes so much sense. I've been trying to make a W or F sound with my lips completely closed and with a total stop of air flow all weekend. It hasn't worked. At all. Not even a bit. :-)